iCLM Model for HIV, TB & Malaria
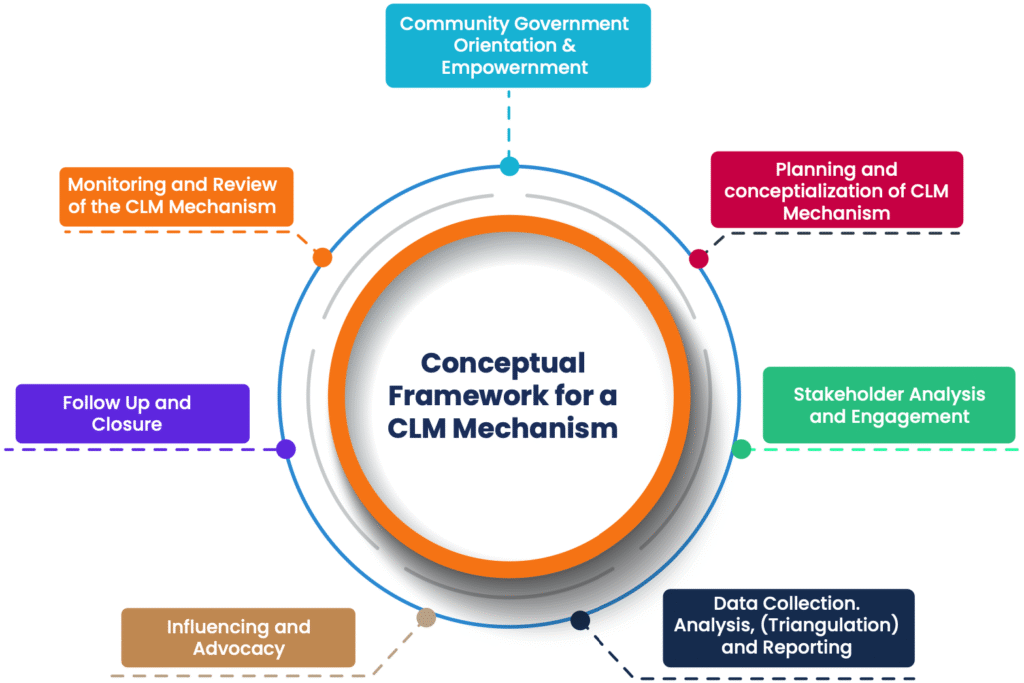
I. Community and Stakeholder Orientation and Empowerment
This is a foundation step in the design of any CLM model that seeks to introduce and even out the definition and understanding of CLM amongst all stakeholders; and empower them on what CLM is, its objectives and outcomes, and what it is not. This is a critical process that will go on throughout all the other steps, and it allows stakeholders to engage and participate in all the subsequent steps from an informed perspective. A series of stakeholder orientation and empowerment meetings have been undertaken at various levels, with some of the meetings and workshops undertaken with the support of UNAIDS and PEPFAR.
II. Planning and Conceptualization of the iCLM Model
III. Stakeholder analysis and engagement
A collaborative stakeholder analysis and engagement approach has been adopted, has started and will continue throughout the implementation of the iCLM model. Stakeholder analysis and engagement are the cornerstones for building a successful and sustainable iCLM model for HIV, TB and Malaria. By fostering collaboration and communication between all stakeholders, the model can empower communities, strengthen healthcare systems, and ultimately pave the way for a healthier future.
Stakeholder analysis and engagement will be undertaken at the onset of the iCLM model design. The analysis and engagement will be undertaken at national level, in targeted health facilities and at community level. The analysis and engagement will encapsulate all stakeholders including those from community based and KP led organizations and communities themselves; the RBC, the HIV, TB and Malaria programs and the Rwanda CCM; technical and funding partners including but not limited to PEPFAR, UNAIDS, the Global Fund, the Roll Back Malaria (RBM), the World Health Organization (WHO), and the Stop TB Partnership.
IV. Data collection, analysis and reporting
Data collection is conducted at both health facility and community levels using digital tools tailored for HIV, TB, and Malaria. Trained community monitors administer four tools: a health facility service user tool, a community-based service user tool, a fortnightly health facility staff tool, and an observation tool. These tools are configured on tablets or Android devices and translated into English and Kinyarwanda to ensure usability. Community monitors are selected based on language skills, local residency, and familiarity with digital devices, and they are trained on tool usage and data gathering methods.
Analysis is carried out using locally developed software aligned with the iCLM model. Real-time data analysis allows for daily issue identification and response. Monthly reports summarize findings from the five pilot districts and guide the steering committee’s interventions. Quarterly reports are shared at formal district and national dissemination meetings. Reporting also includes community feedback sessions and open-access platforms to enhance transparency, inform stakeholders, and promote evidence-based advocacy.
V. Influencing and Advocacy for the iCLM Model on HIV, TB and Malaria
Influencing and advocacy aim to drive corrective action based on issues identified through data collection. Steering committees at district and national levels review monthly reports to determine key challenges requiring intervention. These challenges form the basis of an advocacy agenda, with tailored strategies and time-bound action plans. Advocacy efforts will involve meetings with health facility and community leaders, engagement with national programs, and collaboration with funding and technical partners. The process ensures that data insights lead to real-world improvements in HIV, TB, and Malaria service delivery.
The steering committee collaborates with district and health facility coordinators and communities to interpret findings and take immediate action. Advocacy messages will be customized according to their target—community, health facility, district, or national level—and audience type. These audiences include district health professionals, CHWs, civil society organizations, health service users, key populations, and high-risk groups. National-level targets include program heads, technical officers, RBC, and the Ministry of Health. Technical and funding partners will also be engaged to amplify advocacy efforts and support implementation of improvements.
VI. Follow up and Closure of identified iCLM Issues and Challenges
The follow-up and closure of identified Integrated Community Led Monitoring (iCLM) issues and challenges should be systematic and thorough. Here are the key steps:
Documentation and Tracking: Record all issues, assign responsible parties, and set deadlines in a centralized tracking system.
Action Plan Development: Analyze root causes and create action plans with stakeholder input and required resources.
Implementation: Carry out the action plans with necessary support to ensure proper execution.
Monitoring and Evaluation: Regularly review progress and adjust plans based on feedback and monitoring.
Communication: Keep all stakeholders informed through regular, transparent updates.
Closure: Verify resolution, document outcomes, and formally close the issue in the system.
Feedback Loop: Collect stakeholder feedback and use it to improve future iCLM processes.
VII. Monitoring and Review of the iCLM
Close attention and stock taking of the aspects of the pilot iCLM that work well and the aspects that need improvement will be undertaken, documented and acted on to facilitate continuous improvement and strengthening of the iCLM model. The learnings may result in modifications and refinement of the iCLM model, revision of strategies, re allocation of resources, adjustment of implementation approaches.
The monitoring and review of the iCLM will be undertaken through structured program review meetings, review and synthesis of M & E reports, and receipt of feedback from all stakeholders engaged in the implementation of the pilot.
The review and strengthening of the iCLM will also inform recommendations generated from this pilot for the scale up of iCLM in Rwanda.